
From Support to Stasis
Optimizing the Transition in Biostasis


The Rapid Cooling Imperative
Biostasis aims to bring the patient into a stable, non-deteriorating state where they can wait for as many decades as it may take before repair and revival may be possible. The speed with which the patient is cooled matters a great deal.
The faster cryonics procedures begin after legal death, the better the outcome. Every delay worsens preservation. The more time that has passed before starting each part of the cryonics procedure, the worse the outcome (all other factors being equal).
Other factors are not equal, however, one of the biggest being the temperature of the patient. (Others being cause of clinical death and the general condition of the patient.) Once circulation ceases, ischemic injury begins immediately. Oxygen deprivation (hypoxia) follows, with the brain being the most vulnerable tissue
The biostasis process consists of multiple stages. To avoid long ischemic delays, it is crucial to have effective and timely standby, stabilization, and transport (SST). During that process, practitioners use cardiopulmonary support (CPS) to maintain circulation and to accelerate cooling. Effective cooling requires immersion in an ice-water slurry with active circulation, not simply packing the patient in ice.
You can see the importance of using proper technique from this well-used chart comparing the cooling rate of three Alcor patients. The “squid” is shorthand for the SCCD – surface convective cooling device – the device that circulates the icy water. The SCCD consists of a system of perforated tubing that circulates the water and emphasizes cooling of the head and areas with major surface blood vessels. Combining cooling with CPS accelerates cooling by moving warm blood from the core of the patient to the surface.
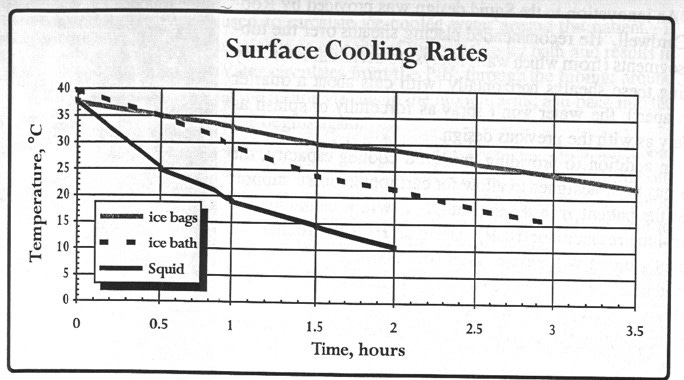
Patients cooled with active circulation and slurry-based methods show dramatically faster temperature decline than passive cooling.
An important transition occurs when a CPS is terminated in order to gain access to the patient’s vascular system. Once completed, the patient can be cooled much more rapidly by passing their blood and cryoprotectants through a heat exchanger. In past practice, this has meant a period during which there is no circulation while surgery is performed and until perfusion can begin. This creates a central operational dilemma: when should CPS be stopped and surgery started?
If you stop CPS at a relatively high temperature you will allow the patient to continue deteriorating at an uncomfortable rate while preparing them for perfusion. Why not cool the patient close to freezing before moving on to the perfusion? But this could take hours. Once the patient is connected to a pump and heat exchanger, they can be cooled much faster. So, at what temperature should you discontinue CPS and move to perfusion?
Why the 20°C Historical Cutoff?
For many years, 20°C was used as the temperature at which to stop doing CPS. A temperature near 20°C is not arbitrary. In conventional medicine, deep hypothermia has long been used during certain cardiac and neurosurgical procedures involving circulatory arrest, where blood flow to the brain and body must be temporarily stopped. Lowering body temperature dramatically reduces metabolic demand and slows the cascade of ischemic injury.
At normal body temperature, irreversible brain injury can begin within only a few minutes without circulation. But as temperature declines, cellular metabolism falls steeply, extending the period during which tissues can survive inadequate oxygen delivery. Clinical experience with deep hypothermic circulatory arrest suggests that temperatures around 18–20°C can permit substantially longer interruption of circulation—sometimes approaching an hour under carefully controlled conditions—while still allowing meaningful neurological recovery.
From the perspective of biostasis, this matters because ischemic injury is cumulative and temperature-dependent. The closer a patient can be brought to deep hypothermic conditions soon after cardiac arrest, the more slowly damaging biochemical processes proceed. Achieving 20°C therefore represents an important physiological threshold: not because injury ceases below that point, but because the rate of deterioration becomes dramatically slower than at normal temperatures. Even if complete vitrification or long-term preservation cannot be initiated immediately, rapidly reducing temperature toward this range may buy valuable time, preserving cellular structure and brain information more effectively until advanced stabilization procedures can begin.
The Role of CPS in Cryonics
Let us take a step back and look at the goals of CPS. First, to avoid misunderstanding, note that we are talking about CPS, not CPR. We are not trying to revive the patient, so it is not “resuscitation.” The goal is not revival, but preservation—maintaining circulation while slowing metabolism.
An effective cryopreservation requires three conditions:
A standby team deployed to the member’s location when risk of legal death is imminent.
Prompt pronouncement of legal death ideally within minutes of cardiac arrest by an independent medical professional. This is typically only possible with in-facility hospice or hospital care.
Restoration of oxygenated blood circulation by high quality mechanical CPS, stabilization medication administration, and commencement of surface cooling no more than ten minutes after cardiac arrest.
If prompt restoration of blood circulation after the heart stops is not possible, cryonics stabilization may consist only of administration of basic medications to inhibit blood clotting followed by several minutes of chest compressions to circulate the medications. This is because restoration of blood circulation after long periods of stopped circulation can do more harm than good.
The goal of stabilization is to maintain viability of the brain by contemporary biological criteria after legal pronouncement of death. To achieve this, four procedures are ideally employed:
Cardiopulmonary Support (CPS). Circulation is restored to provide oxygenated blood to the brain, to circulate medications, and to accelerate cooling. Depending on specific circumstances, the lungs may be ventilated.
Induction of Hypothermia. The temperature of the patient is lowered to just above 0 degrees Celsius to depress metabolism.
Administration of Medications. Drugs are administered to improve circulation, inhibit blood clotting, and to protect the brain.
Blood substitution. If the patient is distant from Alcor’s facilities, and if it is logistically possible to do so, the blood of the patient is substituted with an organ preservation solution to enhance cooling, prevent blood clotting, and protect against cold ischemia.
With current methods, all cryonics patients will suffer some cerebral ischemic injury. The goal is to limit this to no more than the equivalent of a few minutes of ischemia at normal body temperature.
If the top priority is to minimize ischemic injury by restarting circulation and respiration, what is the best way to provide CPS? In terms of effectiveness, the ideal method would be extracorporeal bypass to ensure adequate blood flow. This method suffers from a practical problem, however. It requires invasive surgery to directly access the circulatory system and this takes time, making it typically not a good option for immediate intervention.
The Importance of the Cooling Rate
Historically, at least at Alcor, CPS was terminated when the patient reached a core temperature of 20 degrees Celsius. Above that temperature, CPS was continued to prevent ischemic injury during preparation for blood substitution or cryoprotective perfusion.
Around 2013, Dr. Steven Harris, at the time Alcor’s medical director, suggested modifying the 20 °C cutoff by making it dependent on the rate of cooling. This change acknowledges that a fixed rule is not optimal. A patient who is larger – especially if this is due to adipose tissue – or who has poor circulation will cool more slowly. Since surgery for perfusion will take time during which there is no circulation, the patient should be cool enough to substantially slow metabolism. On the other hand, once surgery is completed, cooling can be greatly accelerated. If a patient is cooling rapidly, they may be taken down to 20 °C or even 15 °C. If they are cooling slowly, CPS may be terminated at a higher temperature.
We can estimate metabolic rate by means of the Q10 rule (metabolism slows by about 50% for each 10 °C drop in temperature) and the Arrhenius equation. This led to Dr. Harris’s recommendation: a simple rule for determining when to continue cooling: Determine the patient’s temperature, divide by 300 (minutes), and the result is the cutoff cooling rate. Examples:
For 30 C, the cutoff is 30/300 = 0.10 °C/min
For 25 C, cutoff is 25/300 = 0.083 °C/min
For 20 C, cutoff is 20/300 = 0.067 °C/min
For 15 C, cutoff is 15/300 = 0.05 °C/min
Some people reflexively push back against this rule – especially those new to the field – because they believe their surgeons can complete surgery in just a few minutes. Such beliefs have typically not been substantiated. As a result the patient is exposed to prolonged ischemic arrest during surgery.
Measuring Ischemic Damage: e-HIT and S-MIX
Using a cooling-rate adjustment to the 20° C rule is one way to reduce ischemic damage.
How can ischemic damage be quantified? One minute or one hour of damage at close to normal body temperature will be much worse than the damage during the same time at 5 °C. Steve Harris developed a time-equivalent index number, or “E-HIT.” Aschwin de Wolf and Michael Perry refined this idea into the S-MIX score: a Standardized Measure of Ischemic eXposure. I will not go into the details here but you can find more information here and here.
Practical Challenges
Two practical challenges present themselves. The first is one I experienced firsthand in Alcor’s operating room. Those involved in the procedure knew of Dr. Harris’s equation but tended to default to the simple 20 °C criterion for stopping CPS. Several times, I had to remind them to use the equation. Since I was overseeing procedures and did not have to focus on a specific task, I would also compute the cooling rate and call out when we were getting close to the CPS stopping point. Although I printed out the equation and related information and put it in the OR, I am not sure that it is being used. This underscores the value of having a dedicated protocol overseer.
The other challenge relates to surgical capabilities. Ideally, surgery would be performed without interrupting circulation. This removes the trade-off between continued cooling and early cessation of CPS and initiation of perfusion and accelerated cooling. Doing this requires a surgeon who can perform surgery with minimal interruption of circulation. At Alcor, that turned out to be difficult to achieve in practice. I do not know whether Alcor has mastered that practice.
Tomorrow Biostasis recognizes this issue and is changing its protocol to incorporate cooling rates. They have been using the same default cut-off of 20°C but the team leader can decide to start higher or lower based on two factors: cooling rate and estimated time for surgery. According to CEO Emil Kendziorra, Tomorrow’s standard procedure going forward “is to start with femoral cannulation and perfusion via the femoral artery during CPS. And then add aortic cannulation a bit later at lower temperatures. This combines the best of both worlds and has the added benefit of a better flow gradient across the brachiocephalic trunk and left subclavian.”
Conclusion
The question of when to terminate CPS is not a minor technical detail—it is a central optimization problem in biostasis. Every decision in this narrow window trades off ischemic injury against the opportunity for faster cooling and more effective perfusion.
What emerges from this analysis is a broader lesson: fixed rules are rarely optimal in a system as dynamic and variable as human physiology under emergency conditions. The traditional 20 °C cutoff is simple, but simplicity comes at a cost. By contrast, incorporating cooling rate, surgical timing, and metabolic modeling allows for decisions that are responsive to the actual condition of the patient.
Metrics such as S-MIX push this further, offering a way to quantify what was previously intuitive: total ischemic burden. With better measurement comes better optimization—and, ultimately, better preservation.
One way in which Biostasis Technologies is working to reduce the gap between stabilization and washout cooling rates is through liquid ventilation (LV). LV has been a work in progress for years, even decades. Recent BT work lead by Charles Platt looks close to being a deployable new procedures that can reduce S-MIX scores.
As cryonics advances from a largely procedural discipline toward a data-driven one, these kinds of refinements will matter. Small improvements in the transition from support to stasis may translate into large differences in the recoverability of the brain.
In a field where success depends on preserving information over decades or centuries, optimizing these minutes may be among the most important work we do.