


Photo by Volodymyr Hryshchenko on Unsplash
Summary
This essay argues that while the FDA does not recognize aging as a disease, framing it as a syndrome may provide a practical regulatory pathway for clinical trials. Drawing on precedents such as frailty and metabolic syndrome, it outlines how aging could be defined with clear criteria and supported by validated biomarkers like epigenetic clocks. Such an approach could enable trials to target the biology of aging indirectly while still using outcomes the FDA accepts.
Aging is a massive problem. We urgently need to understand it and control it. In the current regulatory environment, this has proven to be difficult.
In my previous essay, I examined arguments for and against classifying or framing aging as a disease. I found that most arguments against treating aging as a disease are weak. Two arguments against treating aging as a disease were harder to dismiss. First, aging may be too complex and multifactorial to fit traditional disease models. Whereas exemplary diseases often have specific causes, aging is comprised of numerous degenerative processes and is systemic. Second, and especially important from the point of view of funding and clinical trials, aging is hard to define. Unlike diseases with defined criteria, we have no single diagnostic marker or endpoint.
Many of my fellow anti-aging, prolongevity friends and colleagues want to see aging officially classified as a disease. In the United States, the Food and Drug Administration (FDA) generally only recognizes as suitable for clinical trials treatments that tackle a specific disease. Without that recognition, the FDA will not approve a trial and that means it will be hard or impossible to raise funds to do research and develop a treatment.
Is there another approach? One that will open up funding and FDA recognition? Before suggesting an alternative approach that might satisfy both anti-aging advocates and government bureaucrats, we should first see what we can learn from an existing trial that some see as a change in FDA policy.
TAMEing the FDA
The Targeting Aging with Metformin (TAME) study is a clinical trial whose design was agreed to by the FDA in 2015 that aims to show that aging can be targeted head-on, by testing whether the diabetes drug metformin can delay the development or progression of chronic diseases associated with aging. These diseases are cardiovascular disease, cancer, cognitive decline, and so on.
Notice that TAME does not present itself as an anti-aging trial. The FDA will not accept clinical trials with “slowing aging” itself as an endpoint. Instead, trials must target a recognized medical condition. The time to occurrence of any of several age-related chronic diseases is this trial’s primary endpoint. The designers of the trial (Nir Barzilai and colleagues) strategically packaged “aging” into a composite clinical endpoint built out of conditions the FDA already recognizes.
TAME does not indicate a formal change in FDA policy. The FDA did not suddenly decide to recognize aging as a disease. Instead, the TAME team worked within the FDA’s existing framework by proposing a multi-morbidity endpoint that regulators accepted as legitimate. In other words: TAME is ingenious regulatory engineering rather than an actual change in FDA classification.
The bad news is that the FDA did not make a blanket exception for anti-aging. Three features made TAME acceptable:
A well-characterized, safe drug (metformin) with a long track record.
Endpoints framed in terms of recognized diseases, not “aging.” The FDA recognizes those diseases individually, and so it can approve a trial that measures whether metformin reduces the risk or delays onset of any of them.
Strong advocacy from respected researchers and organizations.
Even if TAME was motivated by anti-aging goals, it was not presented in that light. Other anti-aging trials would probably be rejected because the FDA has no disease code or regulatory framework to approve it. One intriguing feature of TAME lies in one of the two endpoints. The first is Type II diabetes, which is a perfectly standard endpoint. The other is a bit more interesting: development or progression of age-related chronic diseases—such as heart disease, cancer, and dementia. This second endpoint is not a single disease but is much broader.
TAME does not reveal a real shift in FDA thinking. It does suggest the importance of multiple endpoints tied to observable health outcomes.
Well, that makes it easy to present aging for clinical trials, right? All researchers need to do is to measure biomarkers such as telomere length, epigenetic clocks, and proteomic signatures. Problem solved!
Alas, the FDA does not currently accept those biomarkers as validated clinical endpoints.
TAME does not reveal a real shift in FDA thinking. It does suggest the importance of multiple endpoints tied to observable health outcomes.
To be an agency-acceptable endpoint, a measure must be strongly and consistently linked to meaningful patient outcomes such as reduced morbidity or mortality. Telomere length, for example, correlates with aging but is not yet accepted as a surrogate endpoint. So, a company could propose a trial to lengthen telomeres or shift DNA methylation clocks, but unless they tie this to fewer heart attacks, less cancer, or longer disability-free survival, the FDA wouldn’t recognize it.
What is a disease?
Nosology – the classification of diseases – divides conditions into disorders, diseases, syndromes, lesions, and injuries. The term “disease” refers to any condition that impairs the normal functioning of the body. Diseases are generally seen as having only one cause and to classify a medical condition as a specific disease requires knowing its cause, its effects, and the related symptoms. Diseases can be classified and categorized by cause, mechanism (pathogenesis), or by the organ system affected.
I’m not interested in the terms illness and sickness in this context even though they are both frequently used as synonyms for disease. Unless taken to be stand-ins for disease, these terms are even vaguer and illness can simply refer to a patient’s experience of a disease rather than to causal factors or the parts of the body affected. Nor will I dwell on the term “pathology” since it is defined in terms of disease – the typical manifestation or behavior of a disease – and therefore does not help with clarity.
It may seem that there is an easy answer to the question: “What is a disease?” It turns out to be complicated. As Leach puts it: “Most of us feel we have an intuitive grasp of the idea, reaching mentally to images or memories of colds, cancer or tuberculosis. But a look through any medical dictionary soon shows that articulating a satisfactory definition of disease is surprisingly difficult. And it is not much help defining disease as the opposite of health, given that definitions of health are equally tricky.”
Some typical definitions of disease:
A condition of the living animal or plant body that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.
An illness of people, animals, or plants caused by infection or a failure of health.
An abnormal condition of a part, organ, or system resulting from various causes, including infection, genetic defect, or environmental stress.
Aging can be loosely defined as: a disorder of structure or function in a human, animal, or plant, especially one that has a distinctive group of symptoms, signs, or anatomical changes and often a known cause. Apart from the argument against regarding aging as a disease that I considered in my previous essay, some – such as Daniel Belsky, an assistant professor at Columbia Mailman School of Public Health – have suggested that aging is a cause of disease, not a disease itself.
This fits quite well with the point made by many prolongevists: that curing aging would have much greater benefit than curing individual diseases such as cancer and cardiovascular disease. I would not agree with Belsky that this means aging increases vulnerability to disease but is not itself pathological. Better to say that aging is pathological but not itself a disease. I think he is on safer grounding in suggesting that targeting aging processes would be more akin to preventive medicine than disease treatment.
Another perspective suggests that “aging is neither a disease, nor a non-disease. Instead, it combines all age-related diseases and their preclinical forms, in addition to other pathological changes.” Even in the absence of a formal diagnosis of a disease, individuals in their later years will usually show pre-clinical signs of multiple diseases and disorders. The Gladyshevs suggest that “One can say that aging and disease go hand in hand: aging is a key risk factor for human chronic diseases, many treatments and interventions targeting age-related diseases can increase the lifespan of model organisms, and interventions extending organismal lifespan often delay diseases of aging.”
Better to say that aging is pathological but not itself a disease.
The Gladyshev’s view is that the debate over aging as a disease is “false,” by which I think they mean it is what philosophers call a category error. Neither side is correct because the issue is being framed unhelpfully. They suggest we see aging as a “combination of all age-related diseases (in both clinical and preclinical forms) together with other deleterious changes.” Looked at the other way around, “chronic diseases and their preclinical forms (combined with the myriad of deleterious changes not yet pathologized) are nothing but aging.”
The first part of this seems sensible although it leaves a lot of work for “other deleterious changes” to do. The second part seems less helpful. That clause also carries much of the explanatory burden in the second half. Most useful is their underlying point, which is that we should recognize “aging as a combination of diseases (together with other deleterious changes).” Unlike Belsky and others, they do not see the aging-as-natural as conflicting with aging being pathological.
This moves us away from trying to force aging into the “disease” box and instead to see it as a collection of pathological changes including but not limited to diseases. That sounds awfully like aging being a syndrome.
Syndrome?
A syndrome can be defined as:
The association of several signs and symptoms, or other characteristics that often occur together, regardless of whether the cause is known.
A set of medical signs and symptoms which are correlated with each other and often associated with a particular disease or disorder.
A cluster of symptoms and signs that often—but not always—share a common pathogenesis.
One example is Down syndrome which has only one cause (an extra chromosome). Another is Parkinsonian syndrome which has multiple causes. Some syndromes do not have known causes whereas causes have been identified for Down, Wolf–Hirschhorn, and Andersen–Tawil syndrome. In some cases, a syndrome may relate to more than one disease, as in toxic shock syndrome, premenstrual syndrome, and premotor syndrome. When a syndrome is tied to a specific cause it is usually then referred to as a disease. In some cases the terms syndrome, disease, and disorder are used interchangeably because of a close connection between the syndrome and a cause.
Aside from a few single-cause cases, syndromes usually involve a cluster of symptoms with a shared pathogenesis. Examples include metabolic syndrome, frailty syndrome, and post-polio syndrome. Aging, of course, consists of a wide range of symptoms such as muscle loss, immune decline, and cognitive impairment. These do not have a single shared pathogenesis – unless you think programmed aging is the entire explanation for aging. (You could point to “failure to control local biological entropy” but that would be rather too general!) But some recognized syndromes have either unknown or multiple causes.
When I asked both ChatGPT 5 and Grok 4 about aging as a syndrome they said that “There has been discussion in the geroscience community about classifying aging as a “syndrome” of multi-system decline.” When I followed the references, however, I found no mention of syndrome. If readers know of previous framings of aging as a syndrome (or syndromes), please let me know.
Aging as a syndrome seems like a good fit:
Aging involves predictable but variable patterns.
Like metabolic syndrome or AIDS, aging involves multiple interconnected pathological processes.
These processes collectively lead to functional decline and disease vulnerability.
The syndrome framing may avoid the stigma and definitional pitfalls of calling it a “disease” which some have emphasized.
It allows different combinations and severities of aging manifestations among individuals, while still recognizing a treatable clinical pattern.
For FDA purposes, we might refer to “Aging Decline Syndrome,” “Age-Related Decline Syndrome,” or “Degenerative Aging Syndrome.”
Aging as a syndrome has not yet been recognized by the FDA. But the FDA does recognize something fairly similar: frailty syndrome. Frailty is defined clinically as a multisystem decline leading to increased vulnerability (low muscle mass, weakness, fatigue, slow walking speed, and so on). In some contexts – studies of sarcopenia drugs or interventions aimed at older adults – the FDA has accepted frailty as a trial endpoint.
Importantly, frailty is recognized because it can be measured consistently (e.g., Fried’s frailty phenotype, Rockwood’s frailty index) and it correlates with hard outcomes like disability, hospitalization, and death. In other words, frailty syndrome is operationalized and diagnosable: there’s a checklist of clinical signs that define it. That makes it “treatable” under FDA rules.
By contrast, aging is still seen as too broad and heterogeneous — it includes many different biological processes (telomere attrition, mitochondrial decline, immune aging, etc.), and no single validated clinical definition exists. So while frailty is an “aging-related syndrome,” it has a tight enough definition to pass regulatory muster.
The precedent of frailty shows that the FDA can accept syndrome framing when the syndrome has clear diagnostic criteria, it predicts meaningful outcomes, and changes can be measured in trials. If aging researchers can do something similar (e.g., establish “biological age” measures as valid surrogate endpoints, the way HbA1c became accepted for diabetes), then “aging as a syndrome” could become eligible for trials.
The FDA recognizes plenty of syndromes such as frailty, metabolic syndrome, irritable bowel syndrome, acute respiratory distress syndrome, polycystic ovary syndrome, IBS, Tourette’s, and sarcopenia. To be recognized, syndromes must have 1. Clear diagnostic criteria. 2. Predictable clinical course. 3. Measurable outcomes that can serve as trial endpoints.
The precedent of frailty shows that the FDA can accept syndrome framing when the syndrome has clear diagnostic criteria, predicts meaningful outcomes, and changes can be measured in trials.
Trials of drugs and behavioral therapies for Tourette syndrome use reduction in tics as endpoints. In the pediatric neurodevelopmental disorder Rett syndrome, the FDA has recognized clinical trial endpoints such as breathing abnormalities, motor function, and communication. For Prader-Willi syndrome the FDA has allowed drug trials targeting hyperphagia and behavioral outcomes. For irritable bowel syndrome, accepted endpoints are bowel movement frequency and pain scores. For Polycystic Ovary Syndrome (PCOS) – trials target fertility, metabolic symptoms, and hormonal regulation.
The FDA’s acceptance of other syndromes — even when they are multifactorial, heterogeneous, and cluster-like (e.g., frailty, IBS, metabolic syndrome) — shows that in principle, a syndrome framework can work.
This perspective finds support in the WHO’s compromise position of “ageing-associated decline in intrinsic capacity”—recognizing aging’s medical relevance without fully pathologizing it.
What’s missing for “aging” is a set of consensus diagnostic criteria and validated surrogate endpoints. Frailty shows that once those exist, the FDA can incorporate them.
The World Health Organization appears to be ahead of the FDA in that the 11th edition of its International Classification of Diseases (ICD) classifies aging as a medical condition, although not as a disease in the traditional sense. In place of “old age” the WHO uses the term “aging-associated decline in intrinsic capacity.” That is progress! It means the WHO recognizes aging as a treatable medical condition. The WHO is concerned about the implications of treating aging as a disease (for reasons I found less than compelling in my previous essay). With a syndrome framing, that barrier may be lowered. The ICD-11 does include an extension code for “aging-related” diseases, allowing for targeted interventions.
If aging as a syndrome is too big of a pill for the FDA to swallow, we could instead break the aging problem down in several syndromes. Some of these may well be overlapping but separating them might make trial design and FDA acceptance easier.
Composite endpoints and hallmarks of aging
Whether we settle on aging as a single syndrome or a group of syndromes, treatments would be defined in terms of composite endpoints. This would require defining specific, reproducible biomarkers that capture multi-system aging. We would also have to prove that modifying those biomarkers improves healthspan outcomes (not just lab values). Then we would have to get the FDA to accept those markers as surrogate endpoints — something that can take years of validation.
Shifting the FDA’s position will likely be far from easy. The agency prefers endpoints that are clinically obvious and meaningful (heart attack, stroke, death, cancer diagnosis) rather than composite biomarkers.
Biomarkers look promising but are not simple or easy to choose or implement. We need to figure out how these biological age measurements change over time within and between individuals. How do these markers vary between individuals and over time? How can we separate significant changes from normal variation? These questions will have to be answered if aging biomarkers are to be practically usable.
Biomarkers look promising but are not simple or easy to choose or implement.
This and other challenges have been discussed by Jesse Poganik. He points out that “fluctuations in biological age predictions can be associated with factors like major physiological stress and intense exercise.” We also need to determine how interventions cause changes in aging biomarkers. Much work remains to establish the ability of many biomarkers to detect interventions. Poganik adds:
This creates a circular problem: we cannot easily test interventions that target aging without reliable biomarkers that respond to beneficial changes, but we cannot validate the response properties of biomarkers without interventions of known efficacy. Breaking this cycle requires studies that simultaneously test interventions and track biomarker responses, linking molecular changes to hard clinical outcomes like intrinsic capacity, disease incidence, and quality of life.
Another challenge comes from the currently high costs of measuring many biomarkers.
The framework presented by The Hallmarks of Aging appears to be a promising starting point for selecting or finding aging biomarkers or endpoints. The hallmarks are divided into three groups: Primary hallmarks, which are the primary causes of cellular damage. Antagonistic hallmarks, which are antagonistic or compensatory responses to the manifestation of the primary hallmarks. Integrative hallmarks, which are the functional result of the previous two groups of hallmarks that lead to further operational deterioration associated with aging.
Primary hallmarks (causes of damage)
Genome instability
Telomere shortening (or telomere attrition)
Epigenetic alterations
Loss of proteostasis
Impaired macroautophagy
Antagonistic hallmarks (responses to damage)
Deregulated nutrient sensing
Mitochondrial dysfunction
Cellular senescence
Integrative hallmarks (culprits of the phenotype)
Stem cell exhaustion
Altered intercellular communication
Chronic inflammation
Dysbiosis
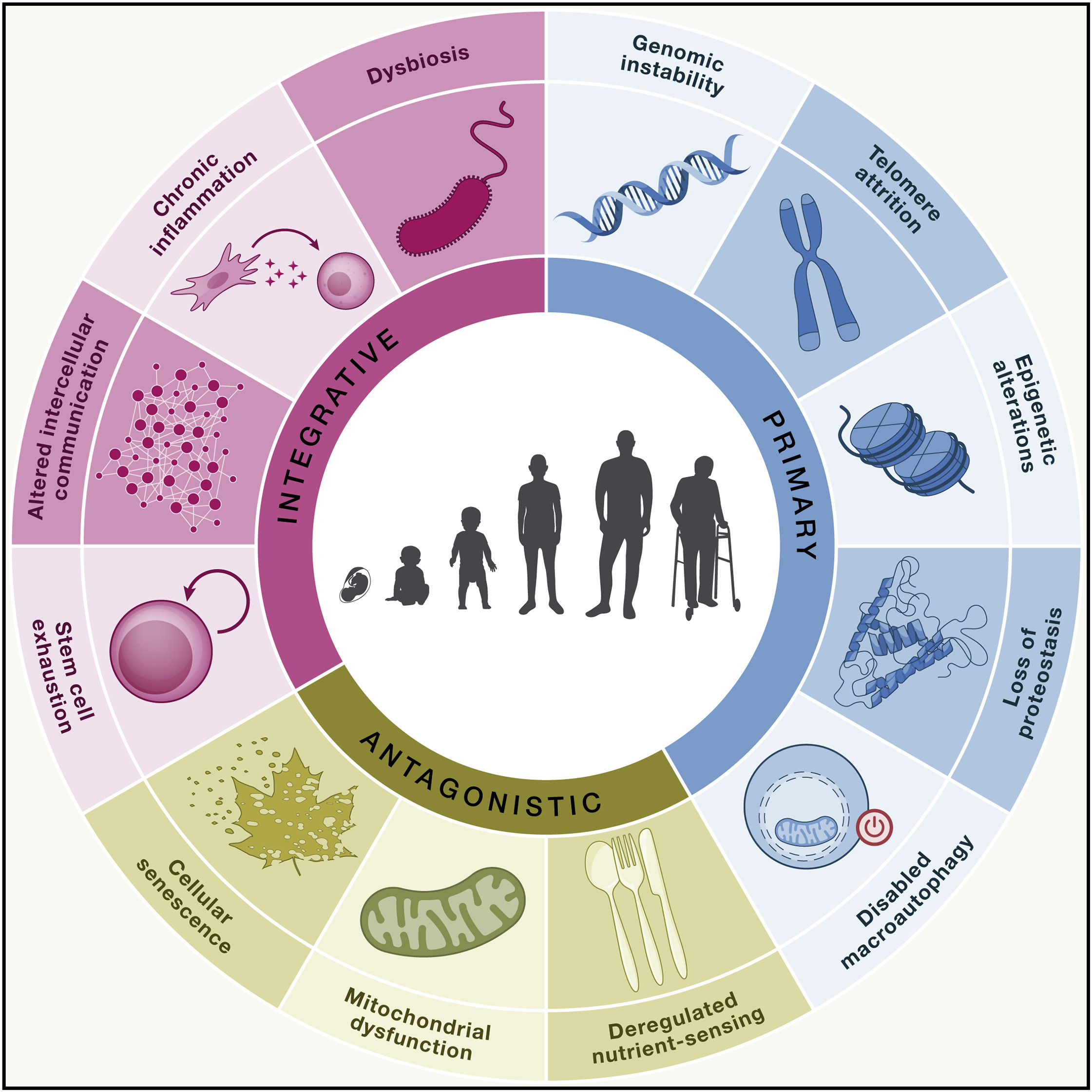
From: Hallmarks of aging: An expanding universe
Possibly, if we are using a multi-syndrome approach, endpoints could be based on these three groups or on each of the 12.
Originally, there were nine hallmarks of aging (2013). The list grew in 2023. A 2025 McKinsey Health Institute report adds two additional proposed hallmarks to bring the total to 14 (although I am skeptical about “psychosocial isolation.”) Even though there are at least two major initiatives to develop effective aging biomarkers, more work is needed especially to ensure that endpoints are clinically helpful.
These hallmarks are not independent of each other. Because they interact there is no one way to classify them. The MHI authors propose three criteria that must apply for each hallmark of aging: (1) the time-dependent manifestation of alterations accompanying the aging process, (2) the possibility to accelerate aging by experimentally accentuating the hallmark, and—most decisively—(3) the opportunity to decelerate, halt, or reverse aging by therapeutic interventions on the hallmark.
The road to FDA acceptance
I am no expert in designing clinical trials for FDA acceptance. However, here is an outline of a possible roadmap to getting “aging-as-a-syndrome” taken seriously by regulators—mirroring what already works for frailty/IBS. This consists of three layers: (A) define it, (B) validate measures, (C) run trials with endpoints the FDA already accepts while you qualify new ones.
Define a diagnosable syndrome: The goal here is a clear clinical construct with objective criteria and staging—so investigators can enroll it and measure change. This requires constructing a syndrome, identifying core domains, and staging.
Qualify biomarkers the FDA can use: FDA will accept biomarkers once they are analytically sound, prognostic for hard outcomes, and—ideally—surrogate (changes predict clinical benefit). Use the Biomarker Qualification Program (BQP) with a tight Context of Use (COU). This involves analytical validation, clinical validation, choosing an aging “clock” panel, determining diagnostic thresholds, and submitting to the FDA’s CDER’s Biomarker Qualification.
Design trials the FDA can approve now—while building the case: Pair accepted clinical outcomes with biological-age measures to both win today and qualify tomorrow. Select an appropriate population, interventions, and primary and secondary endpoints.
For a more detailed roadmap see the appendix.
Conclusion
To get traction with the FDA on anti-aging clinical trials the most important thing is to have clear endpoints linked to clearly bad health and mortality outcomes. Syndrome framing alone will not solve all the problem because of the current lack of accepted endpoints and biomarkers. Firming up and securing agreement to such endpoints and biomarkers looks like the key step. Reframing aging as a syndrome could play a supporting role. It would make it easier to the FDA by avoiding the need to publicly change its position on aging as a disease.
What do you think? Is the syndrome framing helpful? What else needs to be done to develop and present effective and agency-acceptable clinical endpoints?
Resources and references
The classic 1973 paper on problems resulting from the FDAs additional power to regulate drugs for efficacy: Sam Peltzman, “An Evaluation of Consumer Protection Legislation: The 1962 Drug Amendments” Journal of Political Economy, Vol. 81, No. 5 (Sep. - Oct., 1973), pp. 1049-1091 (43 pages)
McKinsey Health Institute report: “Healthspan science may enable healthier lives for all”
Alex Zhavoronkov, Bhupinder Bhullar: Classifying aging as a disease in the context of ICD-11
Timothy V. Gladyshev and Vadim N. Gladyshev: “A Disease or not a Disease? Aging as a Pathology”
Moqri et al.: “Biomarkers of aging for the identification and evaluation of longevity interventions”
Lopez-Otin, Maria Blasco, Linda Partridge, Manuel Serrano, and Guido Kroemer: “Hallmarks of aging: An expanding universe”
Appendix: “aging-as-a-syndrome” roadmap
A) Define a diagnosable syndrome
Goal: a clear clinical construct with objective criteria and staging—so investigators can enroll it and measure change.
Syndrome construct (“Geroscience Syndrome”)
Multisystem decline driven by well-specified hallmarks (inflammaging, mitochondrial dysfunction, senescence, proteostasis, etc.).
Core domains (each with ≥1 validated measure):
Physiologic reserve/physical function (gait speed, grip strength, SPPB, VO₂-estimates, 6MWT)
Body composition (appendicular lean mass by DXA; visceral adiposity)
Cardio‐metabolic/vascular risk (BP variability/arterial stiffness, lipid/lipoprotein profile, glucose-insulin homeostasis)
Inflammation/immune aging (hsCRP, IL-6, TNFR1/2; immune repertoire diversity, sjTREC)
Cellular/molecular aging (epigenetic clocks, proteomic/metabolomic age, glycan age; telomere length as supportive)
Neurocognitive (MoCA or equivalent; processing speed)
Staging (example)
Stage 0 (Robust): all domains within age/sex-adjusted norms
Stage 1 (At-risk): ≥1 domain abnormal or ≥1 “accelerated aging” biomarker outside threshold
Stage 2 (Geroscience Syndrome): ≥2 domains abnormal or composite biological-age index ≥ predefined cutpoint
Stage 3 (Overt frailty): meets accepted frailty criteria (anchors to existing precedent)
B) Qualify biomarkers the FDA can use
FDA will accept biomarkers once they are analytically sound, prognostic for hard outcomes, and—ideally—surrogate (changes predict clinical benefit). Use the Biomarker Qualification Program (BQP) with a tight Context of Use (COU).
Analytical validation (before clinical)
Cross-lab precision/reproducibility (ring trials) for DNAm/proteomic assays; pre-analytic SOPs (collection, storage, batch correction).
Clinical validation
Show that baseline biomarker predicts incident MACE/cancer/dementia/disability/mortality (multi-cohort replication: UK Biobank, ARIC, MrOS, Health ABC, etc.).
Show responsiveness: biomarker changes track with interventions known to improve outcomes (e.g., structured exercise, BP control, GLP-1RA for adiposity).
Candidate “clock” panel (short list)
Epigenetic: Horvath/Hannum (age), PhenoAge, GrimAge2, DunedinPACE (pace).
Proteomic age (SOMAscan/Olink panels).
Metabolomic age; Glycan age (IgG N-glycans).
Inflammaging index (e.g., IL-6, CRP, TNFR1/2 composite).
Functional age (SPPB, gait speed) as co-primary/secondary.
Diagnostic thresholds (provisional, to be prospectively set)
Biological Age – Chronological Age ≥ +5 years (or population-percentile ≥80–90th for risk).
DunedinPACE ≥ 1.05 (faster-than-normal aging).
Gait speed < 0.8 m/s or SPPB ≤ 9 (established risk cutpoints).
Use z-scored, age/sex-adjusted composites to avoid single-marker brittleness.
Regulatory path
Submit to FDA CDER’s Biomarker Qualification with COUs like:
Prognostic enrichment: identify high-risk “geroscience syndrome” for trials.
Response monitoring: detect pharmacodynamic effect on aging biology.
Surrogate endpoint (aspirational): biomarker change predicts reduced multi-morbidity/mortality (meets Prentice-like criteria).
C) Design trials the FDA can approve now—while building the case
Pair accepted clinical outcomes with biological-age measures to both win today and qualify tomorrow.
Population
Adults ≥50 (or ≥60) meeting Stage 2 criteria; exclude overt, single-disease endpoints dominating near term (to avoid confounding).
Interventions
Senolytics, mTOR/AMPK modulators, GLP-1/GDF15 axis, partial reprogramming (low-dose, transient), exercise mimetics—each with safety monitoring tailored to class risks.
Endpoints (hierarchical/composite)
1. Primary (clinical, FDA-familiar)
Time to first event in a Geroscience Clinical Composite (GCC): incident MACE, incident invasive cancer (ex-NMSC), incident dementia, major osteoporotic fracture, or all-cause mortality.
Alternative: Disability-free survival (death, dementia, or persistent ADL disability).
2. Key secondary
Biological-age change (pre-specified multi-omic composite); DunedinPACE shift; GrimAge2 delta.
Function: SPPB, gait speed, grip, 6MWT; QoL (PROMIS Physical/Cognitive; EQ-5D).
Healthcare utilization: all-cause hospitalizations, ED visits.
Design
Event-driven, randomized, blinded, 2–4 years, with adaptive features.
Platform/umbrella structure to test multiple gerotherapeutics against a shared control; alpha-spending plan for multiplicity; competing-risk models.
Operations
Central labs for ‘omics; pre-registered analysis; batch correction plans; device calibration.
Diversity targets (age, sex, race, socioeconomic) and geriatric safety monitoring (falls, sarcopenia).
Regulatory labeling strategy
Near-term: “reduces risk of major age-related chronic diseases” (via GCC) in defined high-risk adults.
Medium-term: once biomarker qualification is secured, pursue surrogate-based accelerated approval with required confirmatory outcomes.
What success looks like
A case definition with staging that clinicians can apply.
Qualified biomarkers (at least for enrichment/monitoring) via FDA BQP.
Positive RCTs showing reduced multi-morbidity (or disability-free survival) and coherent shifts in biological-age measures.
A path to surrogate endpoint acceptance after prospective linkage between biomarker change and hard outcomes.